lore m. dickey
Gender Confusion Is an Attachment Disorder Tracing Back to the Parent-Child Relationship
In 2019, the American Psychological Association (APA) gave a female-to-male transgender graduate student its prestigious “Award for Distinguished Early-Career Contributions to Psychology in the Public Interest.”
They cite her example as a “distinguished scholar” for her promotion of gender transitioning. The award was announced in The American Psychologist.
In making such an award, APA is sending a clear signal to potential graduate students: anyone entering the field with a different understanding of human nature will not be welcome.
Rejecting One’s Body is Not Normal
Some clinicians, however, do not accept the APA’s transgender ideology. Paul McHugh, M.D. Distinguished Service Professor of Psychiatry at Johns Hopkins Hospital, testified to the Supreme Court that embracing a transgender identity is, in reality, a problematic solution.
“Those who are affirmed in their gender beliefs,” he said, “progress from social transition to surgical interventions at their peril. Indeed, if the evidence shows us anything, it indicates that those who progress all the way through surgery fare poorly….There is little evidence that social transition is the panacea that the American Medical Association makes it out to be.” Dr. McHugh compares transgenderism to anorexia nervosa, where the patient perceives himself to be fat, when in fact, he is thin. Ideology rather than science is driving the A.M.A.’s support for gender transitioning, McHugh says.
A decade or so ago, when transgenderism was listed as a disorder, psychologists viewed the rejection of one’s biological sex as evidence of mental illness.
The American Psychologist details the troubled background of the student who received the award, lore m. dickey (no capital letters). Typical of persons with gender-identity confusion, she describes a traumatic childhood: an alcoholic father who had a secret gay life; she struggled with alcoholism, depression, suicidal thoughts, and lesbianism; and she later determined that happiness, so very long elusive, could finally be found by becoming a man.
When the Boy Seeks a “Defensive Fusion” with the Highly Stressed Mother
But in the classic text Gender Identity Disorder and Psychosexual Problems in Children and Adolescents, Kenneth Zucker, Ph.D. and Susan Bradley, M.D. see the condition not as a path to liberation, but a disorder.
Both clinicians worked extensively with gender-disturbed children. In the backgrounds of males who wished to become females, they often found two types of mothers: those who clung to their sons to form a “blissful symbiosis” so that the boys were unable to understand “where the mother left off and they began”; and another type—the severely stressed, highly anxious woman whose small sons sought to develop a “defensive fusion” with the mother as a means of feeling safer. In these cases the boy had an intense but insecure relationship with a mother who was available only intermittently, and therefore “becoming like Mommy” helped the boy feel secure in an otherwise chaotic home.
The clinicians also found that the child was unusually sensitive— he or she had a “constitutional vulnerability to high arousal in stressful or challenging situations.”
Fathers of gender-disturbed boys were also not typical. They tended to step back and defer to their wives’ decisions, including her tolerance and/or approval of their sons’ feminine behavior.
When Claiming a Female Identity Feels “Unsafe”
In the case of gender-disturbed girls, the two clinicians found that 77% of mothers had a history of depression, and they posited that the girl may have felt an unconscious aversion to identifying with her mother because she perceived her as weak, incompetent and helpless. Either directly or indirectly, the mother communicated to her daughter that being female was unsafe.
With such a traumatic background, the researchers say, “Many girls with gender-identity disorder are preoccupied with power, aggression and protection fantasies.”
Yet rather than penetrating the psychological factors that drove this troubled psychology graduate student, lore m. dickey, into a rejection of her biological sex, the A.P.A. agrees that she is now a man, and presents her with one of its highest awards— and then promotes her into the ranks of their own profession.
Research Finds Disorganized Attachment Style
A journal article published in Frontiers in Psychology (2018,9:60, “Attachment Patterns and Complex Trauma in a Sample of Adults Diagnosed with Gender Dysphoria”) investigated 95 gender-disturbed adults.
The researchers found that “gender-dysphoric adults showed significantly higher levels of attachment disorganization.”
A pattern which emerged with frequency for men was “more involving, and physically and psychologically abusive fathers” while the sons were “more often, separated from their mothers.”
What do These Findings Mean?
The authors of the latest research study are only willing to see these unusual family patterns as “risk” factors and were unwilling to suggest they could be causative of the condition.
However, clinical analysis would suggest that any family pattern which interfered with the child’s same-gender attachment would logically be problematic. In the above-mentioned study, the “involving” fathers could have been narcissistic— that is, fathers who used their children as narcissistic reflections of themselves.
Since these men were also reported by their sons as “abusive,” it would follow that their sons would be inclined to reject them as identification objects. The sons would thus reject the masculinity their fathers represented, and by extension, disown their own masculine bodies, and strive to “be” (i.e., attach to) the mother from whom they had been separated.
In the case of women who believed they were men, the study found more “involving” (potentially “narcissistic”) mothers, with separation from and neglect by their fathers. The autobiography of Chastity (now “Chaz”) Bono, who went from a lesbian identity to transgender, is an intriguing illustration of this pattern.
Psychodynamic Investigation is Abandoned
However, the American Psychological Association is unwilling to look below the surface at causation, which would anger a powerful, internal interest group– the LGBT lobby. They have all but abandoned the classical mandate to “know thyself,” and are now affirming every bizarre condition without asking the first, and most fundamental question of psychology—“Why?”
A January 2021 research paper presented by two psychotherapists is attempting to counter this trend.
“The fantasy that the body can be ‘changed and sculpted’ as a way of being rid of profound psychological problems, needs to come under closer scrutiny,” these clinicians assert. “Patients with gender dysphoria need services that are insulated from overzealous advocacy groups and political activists.”
Stirring testimony from two people who abandoned their attempt to live as the opposite sex, told from a Christian perspective, can be found at https://www.focusonthefamily.com/episodes/broadcast/the-journey-back-to-my-true-identity-part-1-of-2/
—Linda A. Nicolosi
From a man who appreciates the value of a psychotherapeutic approach that respects his deeply held values.
 By Garrett D. Johnson
By Garrett D. Johnson
At an early age, I started hearing the word gay used to describe me. I wasn’t sure what it meant the first time I heard it around kindergarten or first grade, but I could tell it wasn’t good.
The Story of John Paulk
By Joseph Nicolosi, Ph.D.
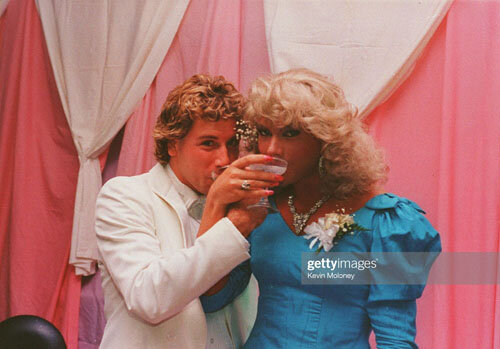
John, wearing the blue dress on the right, in a transgender lifestyle.
Ex-gay spokesman John Paulk left his wife and three sons after more than 20 years of marriage and rejoined the gay community. He has renounced his former married life to a woman and is now discouraging others from attempting change.
Long ago, John emerged from a very troubled past. Prior to his Christian conversion, he assumed an identity as “Candi,” a cross-dressing and drug-using prostitute, immersing himself in the wilder and more anti-social aspects of the gay world. But his Christian conversion led him into a stark change: marriage with Anne, a former lesbian and a committed Christian woman dedicated to an orthodox understanding of family and sexuality, with whom he raised three sons, now teenagers. He also had a key position with Focus on the Family, where he became a well-known media figure testifying to his commitment to heterosexual family life and the traditional, Biblical understanding of sexuality, which holds that a gay identity is a false construct, not part of our human design. But now, all that life has crumbled.
As a reparative therapist who has worked with thousands of homosexually oriented men seeking change, I believe I am in a unique position to speculate on these recent events.
First, John’s story is a cautionary tale about ex-gay celebrity. There is an inherent risk in the ex-gay movement’s reliance on any public spokesperson.
Second, in his testimony, John advises against Reparative Therapy, but he himself has never been in Reparative psychotherapy. Rather, his sexual-identity change evolved as a result of his Christian conversion.
John as a married man in a heterosexual lifestyle.
As John tells his own story, he is a man who always felt unloved and who always searched for identity and belonging. I will not speculate about his own interior processes, because I do not know them. I will, however, speak of psychological patterns I have seen in other SSA (same-sex attracted) men who have gone from “ex-gay” back to “gay” in their lifestyles.
For many SSA men, the deepest problem they must wrestle with is not sexual identity, but core identity. The original source of this struggle is not the more obvious problem in bonding with the father, but a breach in the primary attachment with the mother. For these men, their deepest-level problem is not about sexual orientation but about something more fundamental: identity, attachment and belonging. Gender-identity conflict and attraction to men are only surface symptoms. This is the problem that the media chooses to ignore, and which both sides of the debate fail to acknowledge.
As such a man’s identity evolves, there will be an excited “discovery of my True Self,” followed by disillusionment, then a new “real discovery of my True Self,” and then again, disillusionment. At the base of this desperate search is the anguished grasp for a stable personhood, a profound emptiness and beneath it, a self-hatred. That self-hatred is often expressed in deconstructing and condemning every previous aspect of the person’s own former life, including the influence of persons most near to him.
Radical shifts in “the discovery of my True Self” are associated, in some such people, with Borderline personality disorder, narcissistic personality disorder and gender confusion, since gender identity is built upon an earlier foundation of self-identity. A fragile self-identity makes the later structuring of gender identity particularly perilous.
The restlessness such people feel is shown in a chronic state of dissatisfaction; in the narcissistic expectation that “if others really love me, they must take this pain away from me; and they [or what they stand for] are responsible for my pain.” When others fail to do this, there is a deep sense of betrayal; betrayal that these individuals failed to take away the core emptiness, and so the person in conflict may become angry at the people that participated in his former life. The pain of an identity search and the need for escape from the ordinariness of life can be alleviated for awhile by adulation. The narcissistic inflation found in celebrity, for example, can be an intoxicating balm.

John today, in a gay lifestyle.
This periodic disillusionment leaves behind devastated individuals who have invested deeply in the person; in John’s case, Anne, his wife of 20 years.
The gay community wants to frame changes from ex-gay back to gay as proof that people who experience SSA were simply designed and created for homosexuality, but we would be deceived if we believed this simplistic paradigm.
Where core identity is the foundational problem, we suspect a breach in the primary attachment with the mother. From my clinical experience, there is a particular kind of client who, although he is deeply dissatisfied with gay life and does succeed in developing good heterosexual functioning, will, over time, struggle to muster the self-discipline and maturity to put in a hard day’s work, come home to wife and family, help the children with the homework, have dinner and settle down to a good conversation with his wife, and go to bed. Such a life of day-to-day investment in one’s loved ones seems too confining: it is boring, lusterless, unexciting, “just not enough.” Underneath the boredom and restlessness remains this deep, chronic dissatisfaction.
It’s not just about needing to find a partner of a different gender; it’s about getting attention, flirting, being made to feel special, distracting oneself from one’s chronic dissatisfaction with life through parties and other high-animation activities, such as the gay community offers on its well-known, drug-saturated party circuits. I suspect that “excitement” was what John was looking for when he went to the gay bar in Washington, D.C. many years ago, just after speaking at a Love Won Out conference, when he created a public-relations crisis while working for the ministry Focus on the Family. I don’t believe John was there looking for sex. I suspect he was bored with the Christian community and its expectations – I believe he sought diversion, flirtation, adventure, and – a favored word in gay politics- “transgression.”
Of course, every shift the person makes from “I thought I was such-and-such…” to “Now I really know who I am,” will always have its cheering admirers.
Who is the “real me” — the ex-gay, or the gay man? Each man will decide for himself.
by Joseph Nicolosi, Ph.D.
Homosexual behavior is an attempt to “repair” the wound that left the boy alienated from his own innate masculinity.
See article here:
http://www.crisismagazine.com/2016/traumatic-foundation-male-homosexuality
American Psychological Association Past President Defends Change Therapy
“Contending that ‘all same-sex attraction is immutable’ is a distortion of reality.”

This is what American Psychological Association Past President, Nicholas Cummings, said in a USA Today editorial almost ten years ago–before the media blackout on discussion of such ideas became virtually complete:
(July 30, 2013)– “When I was chief psychologist for Kaiser Permanente from 1959 to 1979…I personally saw more than 2,000 patients with same-sex attraction, and my staff saw thousands more.
“They generally sought therapy for one of three reasons: to come to grips with their gay identity, to resolve relationship issues, or to change their sexual orientation. We would always inform patients in the third group that change was not easily accomplished. With clinical experience, my staff and I learned to assess the probability of change in those who wished to become heterosexual.
“Of the roughly 18,000 gay and lesbian patients whom we treated over 25 years through Kaiser, I believe that most had satisfactory outcomes. The majority were able to attain a happier and more stable homosexual lifestyle. Of the patients I oversaw who sought to change their orientation, hundreds were successful.
“I believe that our rate of success with reorientation was relatively high because we were selective in recommending therapeutic change efforts only to those who identified themselves as highly motivated and were clinically assessed as having a high probability of success.
“Since then, the role of psychotherapy in sexual orientation change efforts has been politicized. Gay and lesbian rights activists appear to be convincing the public that homosexuality is one identical, inherited characteristic. To my dismay, some in the organized mental health community seem to agree, including the American Psychological Association, though I don’t believe that view is supported by scientific evidence.
“Gays and lesbians have the right to be affirmed in their homosexuality. That’s why, as a member of the APA Council of Representatives in 1975, I sponsored the resolution by which the APA stated that homosexuality is not a mental disorder and, in 1976, the resolution, which passed the council unanimously, that gays and lesbians should not be discriminated against in the workplace.
“But contending that “all same-sex attraction is immutable” is a distortion of reality. Attempting to characterize all sexual reorientation therapy as “unethical” violates patient choice and gives an outside party a veto over patients’ goals for their own treatment. A political agenda shouldn’t prevent gays and lesbians who desire to change from making their own decisions.
“Whatever the situation at an individual clinic, accusing professionals from across the country who provide treatment for fully informed persons seeking to change their sexual orientation of perpetrating a ‘fraud’ serves only to stigmatize the professional and shame the patient.”
Nicholas Cummings was president of the American Psychological Association (1979-80).
by Linda Ames Nicolosi
This article first appeared in the National Association of Research and Therapy (NARTH) Bulletin. It is based on an interview with Elaine Siegel, Ph.D., A.D.T.R., a supervising and training analyst at the New York Center for Psychoanalytic Training.
Dr. Siegel lectured extensively in the United States and Europe. She wrote three books, including Female Homosexuality: Choice Without Volition (1988). She passed away in 2013, the same year we interviewed her for this article.
————————
Much has been written recently about lesbianism from a gay-advocacy viewpoint. Therefore Dr. Siegel’s psychodynamic insights— approached from a different perspective— are of special and unusual interest.
There are different types of lesbianism, as Dr. Siegel notes, whose origins will be different from the one described here. But the early-developmental trauma model that she describes was the most common pathway she found among her patients. (The other common family pattern described by clinicians: that of a mother who is the object of abuse, leading the daughter to reject the embrace of a feminine identity as representing weakness, and feeling “unsafe.”)
In Female Homosexuality, Dr. Siegel describes the families of her lesbian patients. Many of these patients had evidently been raised by narcissistic mothers, whose controlling influence attempted to force the fragile, emerging selves of their daughters into an identity that was alien to them. As a result of this disturbed relationship, the daughters, who had been unable to identify with the feminine, developed a severe body-image distortion.
“[M]others,” she says, “seemed to use their children as sometimes desperately needed, sometimes desperately repudiated extensions of themselves…When these little girls tried to turn to their fathers, they did not fare much better. Preoccupied with their business deals, the men sporadically paid attention to their daughters, overstimulated them, and then appeared to forget that they were around…These fathers, when they took the time to react at all, responded to their daughters as persons who had to be made over in their own, masculine image.” (She described one father who tried to make his daughter “fearless” by taking her for a ride on her sled while it was tied to the back of his car.)
Dr. Siegel says, “I have given these accounts to underline that my patients grew up in atmospheres that substituted empty facades for reality, and that tried to force their emerging identities into rigid, idealized forms of behavior alien to them,” with a resulting “severe arrest in ego development” despite outwardly well-adjusted personalities.
“Unable to identify with either parent,” she says, “they literally did not know that they were female.”
The mothers are described as immature, emotionally fragile and aloof from the needs of their daughters. They did not treat their daughters as whole and separate persons, but as extensions of themselves who were expected to fulfill the mother’s needs, not their own. In adulthood, their daughters, having been unable to identify with femaleness, sought to repair their defective body images by seeking a sexual partner similar to themselves.
Because they were unable to integrate their sexual organ into their body image, these women typically developed an unconscious denial of gender differences.
“The little girl who turns to homosexuality never has a chance to create herself. She is a creation of her mother, whose self-love she was meant to enhance,” says Dr. Siegel, paraphrasing M.R. Khan in Alienation in Perversion (1979).
Interview
Q. Dr. Siegel, how did you become involved with the National Association of Research and Therapy of Homosexuality (NARTH)?
A. Many years ago, I sought supervision from the psychoanalyst Charles Socarides. By a series of circumstances, I had a large group of homosexual women in treatment, but at that time, I was unfamiliar with lesbian dynamics and not sure how to proceed.
Q. Did this supervision help?
A. Absolutely. I had been aware that females became homosexual for different reasons than males, but not much in the literature prepared me for actually treating female homosexuals. As Dr. Socarides and I worked, I understood that lesbianism was due to a developmental lag. In other words, I discovered that female homosexuals–at least the ones I was treating (I’m sure there are different kinds) had a specific type of distorted body image. They did not appear to have appropriate feelings in the vaginal area; that was not an erotic zone for them. Of course, they will hotly dispute this fact, and cite reasons why they really do enjoy foreplay and sexual play. But I found, rather, a profound anesthesia of that whole region.
The interesting thing is that I had no preconceived notion about female homosexuality. I was a “modern woman”; I had believed that homosexuality was just another “way of being in the world” until I started to work with these ladies. They surely taught me differently.
Q. Can you tell me how you got started in the treatment of lesbianism?
A. I started to work with these women because I had belonged to a feminist consciousness-raising group, and one of these women opened a Women’s Center for treatment. She asked me if I would be one of the treating therapists. And, I said, of course; and very soon, I had a whole practice full of women who were really suffering. They were not happy with their lives, and they came into treatment specifically because they wished for a longterm relationship, but were unable to have it.
Q. With a man?
A. No. They just wished for a longterm relationship. They did not specify male or female. I tried hard to keep my analytic neutrality toward my patients’ sexuality. I felt, and still feel, that the analysand herself has to decide whether she wishes to be hetero- or homosexual.
When one thinks about homosexuality, one has to realize that a woman’s first love-object is most often her mother. In my group of analysands, the wish toward objects was most often for a tender, empathic mother who was visible in the transference. These wishes are at first unconscious, but as treatment progresses, wishes toward significant others become conscious in the transference. These wishes belonged to a very early developmental phase.
Early “castration anxiety” [i.e., fear of the power of the avenging mother] distorts the female body image, resulting in panic states due to the unconscious fear of the annihilation of self and other. Essentially sensuous wishes and needs then become sexualized, sometimes resulting in female homosexuality.
I had to be careful not to let my own opinions about homosexuality interfere with their growth. If I had not stayed empathic toward these early needs, my analysands would have been unable to tolerate further analytic investigation.
And if this early phase, which is in essence homosexual, is not traversed, then love for the father–which will lead to heterosexuality–becomes difficult.
Q. So they didn’t really give you any indication of what type of longterm relationship they were interested in?
A. Correct.
Q. And they didn’t indicate whether they were homosexual or not?
A. Correct; but they seemed anxious about their sexual orientation, and if they saw themselves as homosexual, I thought, well, OK, you’re homosexual. Now interestingly, there were a couple of women who did not start homosexual behavior until after they were in the treatment, where their transference–or the flight from it–made them feel safe enough act it out.
Later, upon analyzing their behavior, they gave it up. It had been a regression in the service of building themselves up because when they were in therapy with me, I could work with them and talk about these options…how and why they had to stimulate themselves in an unusual manner. I found it extraordinary how many of them had ugly names for their vagina. They called them “stink holes,” and they were not pleased with this part of the body–as opposed to males, who are usually very pleased with their penises.
Q. How did this negative body image arise?
A. Invariably, it was a faulty mother-daughter relationship. Often the mothers were very narcissistic and didn’t allow themselves to be role models for the daughter.
Q. And so, the daughters could not assume a female identity?
A. That’s right. Because they felt the mothers were either too seductive or too intrusive, or didn’t pay any attention to them at all. It was always a disturbed relationship of some sort. Very often, the mothers appeared to be–at least in their daughter’s view–terribly narcissistic.
The tragedy was that when these children turned to their fathers, the fathers also used the children for their own aggrandizement. When their daughters didn’t go along with this, then the fathers would be disappointed and drop the girls emotionally on their heads, just like their mothers had. So, these were really tragic life histories.
These patients’ neediness was manifest in their demanding (among other things) of body contact from me. When I declined, they were very offended. I had to explain to them that I was not there to gratify them, but to help them look at their lives so they could make healthy decisions.
Yet, I kept myself as available as I could, and put up with four o’clock in the morning telephone calls. There was all sorts of acting out from them, but slowly we went forward. Now, the interesting thing is that even though some of the women did not turn heterosexual through therapy, they still made large gains. They no longer had to use these bizarre techniques to stimulate themselves such as using nipple clamps, tying each other up, and so on. They became happier and more fulfilled people–although they panicked at the idea they might turn heterosexual.
Q. Really, it’s that threatening?
A. Oh, yes. And the other thing that was very difficult for all of the women–they had a lot of trouble with their “lesbian sisters.” They were told by them that they were betrayers, that they were evil, that they were letting the women down, and why did they go to this awful therapist, Dr. Siegel, who “kills homosexuals,” you know, this kind of nonsense.
Q. Kills homosexuals? That was the expression that was used?
A. Yes. When I gave a speech at the New York Institute for Psychoanalytic Training, there was a group of homosexual women who had placards that read, “Elaine Siegel kills homosexuals.” And I tried to get into a dialogue with them, but it was impossible. Their tactic was to disrupt the proceeding, and they did.
Q. Of all the homosexual women you’ve worked with, how successful were you in helping them to acquire a heterosexual identity?
A. More than half. At least 70% decided to at least give heterosexuality a try. Now, you see, if you look at this from an analytic angle, some of them started to live heterosexual lives, but still had homosexual fantasies. So, to my mind, the analyses were not finished, but the women thought they were finished.
Q. And did they stay?
A. Interestingly enough, no–not all of them. What they did do, was keep writing me letters and visiting me for Christmas or something. It was almost as though they needed “Big Mama” to bolster their still-shaky identities.
Q. So, the transference remained positive to a certain degree.
A. Of course, but they needed more analytical work when they remained locked into their early trauma.
Q. That is a terrific success rate.
A. Oh, yes. But I attribute the success to the fact that I really didn’t ever allow myself to think: you must turn heterosexual. When there was a flight from the transference into homosexual acting out, I would never, never, never condemn them, but try to understand it from the transferential point of view. And they began to trust me. They all went through phases where they said, “You can’t understand me because you are heterosexual. I bet you’re even married or have a man in your life.” And I had to swallow and think, “You’re right, I don’t know what a homosexual liaison feels like, I don’t.”
Q. So what were their reactions to their own changing feelings in the therapy? How did they express those observations to you?
A. At first, they were terribly anxious. Then they became depressed and sad.
Q. Why do you think the sadness?
A. The sadness was because they had to give up something that to a certain extent, had worked for a long time. You know, people don’t turn to homosexuality because they want to; inner forces compel them to it. This is true for males and females.
But when this kind of a defense and adaptation no longer works, of course a person is going to be upset. And the relief and the joy of a more fully experienced life and body will come much later.
Q. How did the ones that reached that level express those experiences to you?
A. Oh, they would say to me that I was the greatest analyst in the world and they would thank me so much. It was really touching. You know, I’m not supposed to say this–analysts must stay neutral–but counter-transferentially, I was fond of the whole batch of them.
Q. Did they express surprise about what was happening to them?
A. No, no. They were not surprised, because it is a gradual process, you see. It is not an awakening and saying, “Ahha, I am heterosexual now.” They had already gone through sadness, through experiencing a terrible hole in their body image, in which their genitals had been treated terribly…
Q. So they hadn’t been able to identify with their own femininity…
A. But by the time they got to the point of rebuilding themselves and their body image, they already knew that change was happening, so they were not surprised. They were at first angry, then grateful.
Q. Did they ever comment to you on the experience of both worlds, and the difference between both worlds?
A. Yes. You know, it’s very interesting. The ones who had expressed the wish to have a child, were more willing to examine themselves analytically than the others. At the beginning, they had said, “Well, I can always be artificially inseminated.” Or, “Well, I have a very good girlfriend who has a brother, and maybe he would be willing to give his sperm,” or something like that. And I just said, “Uh-huh,” and would wait until we got to a less volatile place where we could discuss that. When they were ready, we would discuss what it would be like to raise a child without a father. Or what it would be like to raise a child with two mommies. And, as I have said in my books and articles, these women were intelligent and creative. They understood these things.
Q. In recent years, you’ve given seminars in Europe. I’ve heard you had some interesting experiences.
A. Well, when I was speaking at a mental-health association meeting in Sweden, a good half of the audience were homosexual women. They were surprisingly willing to enter into a dialogue. In other words, they didn’t say, “Dr. Siegel wants to kill homosexuals.” They asked questions like, “Why do you want to treat us? Why do you think homosexuality is an illness?” And I would always say to them, “I don’t think homosexuality is an illness. I think it’s a developmental lag. That’s something quite different.” And, I don’t ask you to come into treatment. You come into treatment voluntarily. Nobody stands there with a gun forcing you.
And they would say, “Why do you want to examine homosexuality? Do you do that with heterosexual people?” And I would say–of course I do; the crux of the matter in any analysis is what a person does with his or her sexuality.
Q. The difference between that audience’s reaction and the American reaction was considerable.
A. When my book appeared in Germany, people were also willing to talk. Interestingly, however, the publisher had a bad experience. He had a large order for the book and then it was returned because the bookseller said, “I won’t have that in my store.” I have not heard of such a situation in the United States.
However as you know, the political situation in the United States makes it almost impossible now to treat homosexuals. Even the American Psychological Association has a large contingent that feels you shouldn’t take homosexuals into treatment if you believe the condition represents a problem in any way.
But as we know, the homosexual who wishes to change–who has an unconscious wish to change–is one of the most misunderstood people in the world today.
Elaine Siegel’s related journal articles include “Severe body image distortions in some female homosexuals” (Dynamic Psychotherapy, vol. 2, no. 1, Spring/Summer 1984), and “The connection between playing and adult love: Reconstructions from the analyses of some homosexual women” (Dynamic Psychotherapy vol. 4, no. 1, Spring/Summer 1986).
Client Choice Under Attack:
Interview with David Pickup, LMFT
by Linda Ames Nicolosi

Testifying Before a State Legislature: David Pickup, LMFT
1. David, you have testified before several State Legislatures about the proposed therapy bans. These laws seek to stop any psychotherapy that might reduce same-sex attractions in minors. What’s your thinking on this?
These bans are, in effect, child abuse.
All of our therapy clients believe that their homosexual feelings were caused by emotional and/or sexual abuse. To address this abuse, I use a program called Reintegrative Therapy, which focuses on childhood traumas. As a byproduct of this therapy, when the trauma is revisited, homosexual feelings are often reduced or eliminated. To deny a child their right to heal these underlying wounds would do nothing but further abuse the child.
Can you imagine a child or his parent walking into our offices who wants therapy for homosexual feelings that are associated with their sexual abuse, and having to tell them that overcoming this trauma might change their sexual attractions— and that any change of homosexual feelings would be illegal? This is nothing short of more abuse.
2. If Joe Nicolosi Sr. were alive today, what would be his thoughts on this situation?
If Joe were here, he would be fighting right alongside the rest of us with his characteristic expressions of scientific integrity, passionate belief in what truly works therapeutically, and expressions of healthy, sarcastic wit. He wouldn’t put up with psychological nonsense.
3. Could you tell us about Sam Brinton, who has been paid by gay-activist groups to go around the country testifying in favor of these anti-therapy bills?
Brinton has given false testimony of the supposed Reparative Therapy he received some years ago as a minor. His parents, who would have been the ones who sent him to therapy, refute his story. Brinton says he was harmed by this therapy but he refuses to state, or “can’t remember,” any of the key details—at what age he went to therapy, the name of the counselor, whether it was a religious or licensed counselor (his story has changed over the years), or the location of his experience.
He now believes he has achieved the “freedom” to be who he really is. [Editor’s note: Brinton, who says he is non-binary, was subsequently charged with three occasions of luggage theft of women’s clothes from airport carousels, and then was fired from his U.S. government job managing nuclear waste.] Brinton is someone who engages in degrading animal-fantasy sex, bizarre cross-dressing, sado-masochistic bondage sex, and even the abuse of women in some ways.
And our lawmakers fell, over and over, for Brinton’s story. No lawmaker attempted to verify his claims, even though we told them they were easily shown to be false. Based on this man’s testimony, state lawmakers voted over and over to ban change-allowing therapy for minors.
4. Why are these therapy bans so dangerous?
A client’s right to therapy that benefits him or her should be upheld by all the major psychological institutions in the world. Instead, it is under siege.
Besides, there is a legal issue at stake—the US Constitutional right to free speech. Supreme Court Justice Clarence Thomas recently gave the opinion (coming out of another case regarding free speech) that banning specific types of therapy was a violation of free speech. In contrast, the 9th Circuit court ruled differently some years ago. As this issue continues to work its way through the legal system, we expect other Federal Courts and the Supreme Court to rule in our favor.
5. How do these bans threaten clients’ rights?
To ban therapy because it doesn’t fit a contemporary political or psychological movement will interfere with client dignity and self-determination. The first ethical goal of all medical or mental health professions is, after all, to do no harm, and these bans will harm clients’ rights to self-determination.
Clients’ rates of depression, anxiety and suicidal ideation will no doubt increase, if such therapy is banned throughout the country. The anti-therapy movement will also lead to the breakdown of scientific authority of the mental health profession and public respect for its research, as the layman begins to recognize that politics, not science, is actually driving their agendas.
6. The LGBT movement is demanding that transgender therapy be available to a preschool child. That child is seen as perfectly capable of making his own decisions about who he is, if he seeks to identify as the opposite sex. And yet a teenager with homosexual feelings is seen as not capable of choosing his own identity if it leads him away from a gay lifestyle. Isn’t this intellectually incoherent?
You have just articulated the exact and gross irony of this situation. This incoherence makes it obvious that the LGBT movement to ban therapy is political, self-serving, and not really directed toward the mental health of children. Children are being used for the irrational and biased agendas of adults. They seek to upend our understanding of gender and sexuality and guide it toward a worldview which ignores our biological design. This has happened in history many times before.
7. Why is it so important to the gay community to stop people from leaving homosexuality?
There are two main reasons for the gay community’s resistance. First, testimony such as my own tends to crack the foundation of the LGBT world view, which would require them to face the traumatic underlying causes of the homosexual condition.
Second, people with same-sex attraction usually hold onto unresolved anger from having been shamed or bullied by family, friends and society from many years past. It would be emotionally unsettling if they weren’t able to transfer these unresolved anger issues onto other people in the present. In short, they need to “pay back” the hurt that was done to them.
This maltreatment for having had homosexual feelings is actually why I have so much compassion for the LGBT community. They deserve our compassion, but that doesn’t mean that clients’ rights should be taken away.
8. What other false testimonies have you seen in government deliberations over the therapy bans?
I testified in Denver in March 2019 where two of the most notorious LGBT activists spread their falsehoods in the senate committee. Yet despite my efforts, that committee passed the therapy ban!
One notorious figure is, as mentioned above, Sam Brinton. The other is Matthew Shurka. I’ve testified in around 20 states over seven years. It’s always the same stories from the gay activists. Every one of these testimonies reports horrendous things like electroshock to testicles, shame-based therapies, and coercive techniques. But these activists never report “who, what, where and when” these alleged acts were committed against them. And the committee members never ask them for corroboration.
If these terrible therapies had actually taken place, don’t you think those men would have sued their therapists? Wouldn’t they have reported them to their licensing boards? Yet none of them have done so.
On the other hand, our own testimonies of the existence of safe and effective therapy can establish actual dates, doctors’ names, and places where clients received effective, professional treatment.
9. Where do you think this is all going to lead?
If the Supreme Court still exists as an honorable, wise and unbiased institution, I believe that it will uphold a client’s right to professional therapy.
But if they do not, the U.S. could be hit by a metaphorical iceberg like the Titanic that sunk long ago. It will be an age of something like fascism.
On the other hand, if our rights are upheld in the courts, I believe a new era of professional therapy will emerge in our country that informs everyone that no one has to be LGBT.
10. The Democrats have been unified in favor of the anti-therapy bills. In fact, didn’t Hillary Clinton say she hoped to ban therapy for adults as well?
Yes, Clinton indeed pushed for the therapy bans, even for adults. But in many states there is immense pushback from truth-seeking Republicans. However, in almost every one of the 15 states that have banned therapy, they’ve only succeeded because they are the most liberal states in the Union. From this point forward, it’s going to be very hard for LGBT activists to take hold in many more states to ban therapy.
11. Do you think the legislators you speak to, are actually interested in the truth?
Yes, the conservative ones are, for the most part, but the liberal ones probably couldn’t care less. In my opinion, there is a national dumbing-down of reason, and a blindness to truth.
The Left tries desperately to convey compassion for all diverse peoples. However, compassion without truth degenerates into mindless sentimentality. In fact, compassion just becomes “sentimental niceness” whenever it is not grounded in the truth.
by Joseph Nicolosi, Ph.D.
During the course of therapy with same-sex attracted men, when the client is working on increasing his attraction to women, we sometimes encounter a block to the development of heterosexual intimacy which traces back to the boy’s childhood experience with an intrusive and over-intimate mother. The following are some examples.
A client and I were doing Body Work on an attractive female image. As he gazed at the photo, he felt himself slowly developing warm, close feelings. But just as he was beginning to enjoy the pleasant sensations in his body, he hit a sudden block. He felt a rigidity in his chest (i.e., fear). When we analyzed the problem, a jolting memory came up of his mother “playfully treating me like baby” by taking her breast out and putting it to his mouth. He was 10 years old—a preteen at the time—and the incident, which was supposed to be a joke, had brought up alarming, incestuous feelings at that time which he had felt an anxious need to suppress. In fact, he had “forgotten” those feelings until this moment.
Another mother who was a midwife in a small town, was called to help with a birth, and she took her 7-year-old son (now my adult client) along with her. The mother allowed her son to watch the delivery, and to this day, my client recalls the vivid image of the pregnant woman’s bloody vaginal area and of her terrified screaming. This early, and (to him) horrifying experience of a woman’s body created an association that he was unable to erase. From that time forward, he felt a sense of revulsion regarding the female body.
Another client told me of an incident when he was about 13. He was talking to his mother about his anxieties regarding having a girlfriend, and his inexperience about what to do or say. The mother suggested that the two of them— mother and son—practice kissing together. This client did not need to read Freud to see the connection between that incident and his feelings of apprehension toward women. His mother’s total disregard for normal mother-son boundaries had formed a barrier which prevented the client from developing normal heterosexual feelings. By default, he turned to the “safety” of homosexuality.
Many clients tell me that they and their mothers showered together. The mothers thought such an experience would make their sons feel relaxed about the human body, but instead, they produced the opposite effect. Other clients remember disturbing memories of their mothers walking around the house naked, an image which left them with defensive feelings of abhorrence. Some mothers also insisted on frequent cuddling and hugging, even as their sons got older.
In such situations, the feminine body becomes not a mysterious attraction, as it does for heterosexual men, but rather it becomes an object of dread. For the man who develops homosexually, the male body, in contrast, has no negative childhood associations of boundary violations and therefore, it represents a “safe haven” from the intrusive feminine.
Mothers who are flirtatious with their sons in an erotic manner are seeking to meet their own needs, to the neglect of their sons’. Their motivations could range from mere careless naiveté, to desire for narcissistic gratification, thus turning the son into a sort of plaything and failing to acknowledge his masculine dignity.
Mothers must always be sensitive to the healthy physical and emotional boundaries that are required by the young boy to develop heterosexually. To the male, the feminine must always be mysterious and “other than me,” rather than intrusive, controlling, over-familiar, and suggestive of the threat of incestuous attraction, as so many of our homosexual clients report from their childhoods.